|
Cycle's Approach Background:
In Cycle 1, all patterns determined from the assessment are presented consecutively. This cycle contains between three and six different patterns of phonemes. Target one pattern intensively for a fixed time then move onto the second pattern (even if the child has not mastered the initial pattern or error sound), then moving on to the third pattern and so on until all initial primary patterns of error have been worked on, marking the completion of one cycle. Cycle Example (30 minute sessions 2x a week) Targets: Final Consonant Deletion: CVC Final Nasals: Final M (Session 1 & 2), Final N (Session 3 & 4). CVC Final Voiceless Stops: Final P (Session 5 & 6), Final T (Session 7 & 8). Fronting: Final K (Session 9 & 10), Initial K (Session 11 & 12), Initial G (Session 13 & 14) S blends: SP Initial cluster (Session 15 & 16), SM cluster (Session 17 & 18). Goal of the Cycles Approach:
Ideal Candidates for Cycles:
Choosing Targets: The order of phonological patterns within cycles is based on developmental and clinical phonology research findings and on each individual's phonological abilities. Remember, we are not targeting individual phonemes, but rather entire sound patterns. The clinician should select the client’s most stimulable sounds or patterns, so that the child can experience immediate success. Stimulate any non-stimulable sounds for a few minutes during sessions until they become stimulable (& always facilitate liquids if they are not stimulable). The targeted patterns within the cycle are used to stimulate emergence of a specific sound or pattern in spontaneous language, not mastery of it. Target only those that are consistent deviations and errors that occur at least 40% of the time. Primary First Cycle Targets:
Advanced Target Patterns:
Session structure:
3 & 4 year olds (Rhyming and Alliteration, Segmentation, Blending and Manipulation of words and syllables as well as phoneme and grapheme awareness) 5 & 6 year olds (Onset/Rime and Blending, Segmentation, Blending and Manipulation of phonemes as well as grapheme and phoneme correspondence). Important Components of Cycles: Focused Auditory Input:
Facilitative Contexts:
Optimal Match:
References:
Rudolph, J.M. and Wendt, O. (2014). The efficacy of the cycles approach: A multiple baseline design. Journal of Communication Disorders, 47, 1-16. Evaluating and Enhancing Children's Phonological Skills; A Systematic Approach by Barbara Williams Hodson, PhD, CCC-SLP CEU Bauman-Wängler, Jacqueline A. Articulatory and Phonological Impairments: A Clinical Focus. Boston: Pearson, 2012. Print. Williams, A L, Sharynne McLeod, and Rebecca J. McCauley. Interventions for Speech Sound Disorders in Children. Baltimore: Paul H. Brookes Pub, 2010. Print.
2 Comments
STEP 1: Open up a new blank document in Powerpoint. Keep in mind you can change the layout from landscape to portrait if necessary.  STEP 2: Open up the PDF document that you want to make interactive. This example was bought and downloaded from Teachers Pay Teachers and opens up in Adobe Acrobat Reader  STEP 3: On the bottom left corner of your PC laptop, click the magnifying glass and search the computer for “Snipping Tool”  STEP 4: The Snipping Tool box will pop up in the upper right hand corner. Click “New”. From here, left click and hold while you drag your mouse over the area or picture that you want to snip. 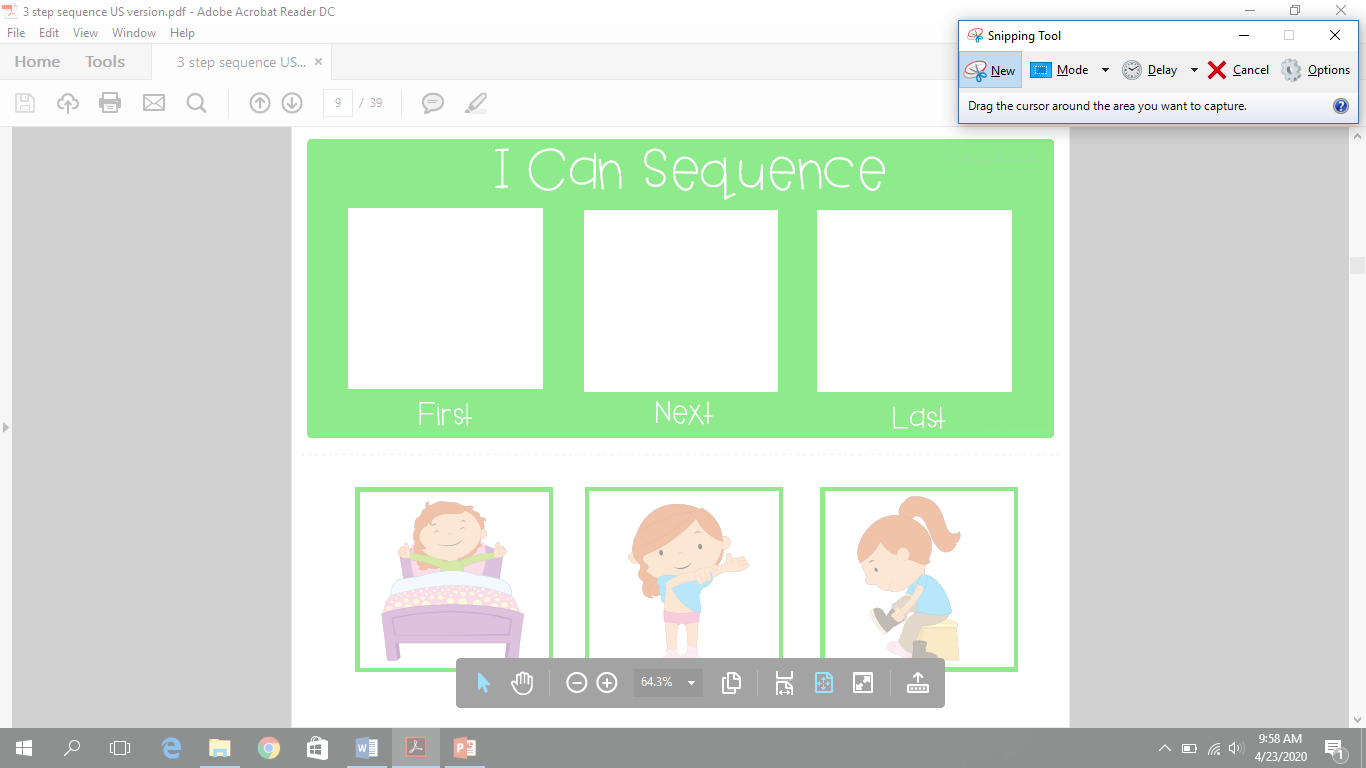 STEP 5: Once you have completed this, a new window will automatically pop up with the portion of the PDF that you snipped 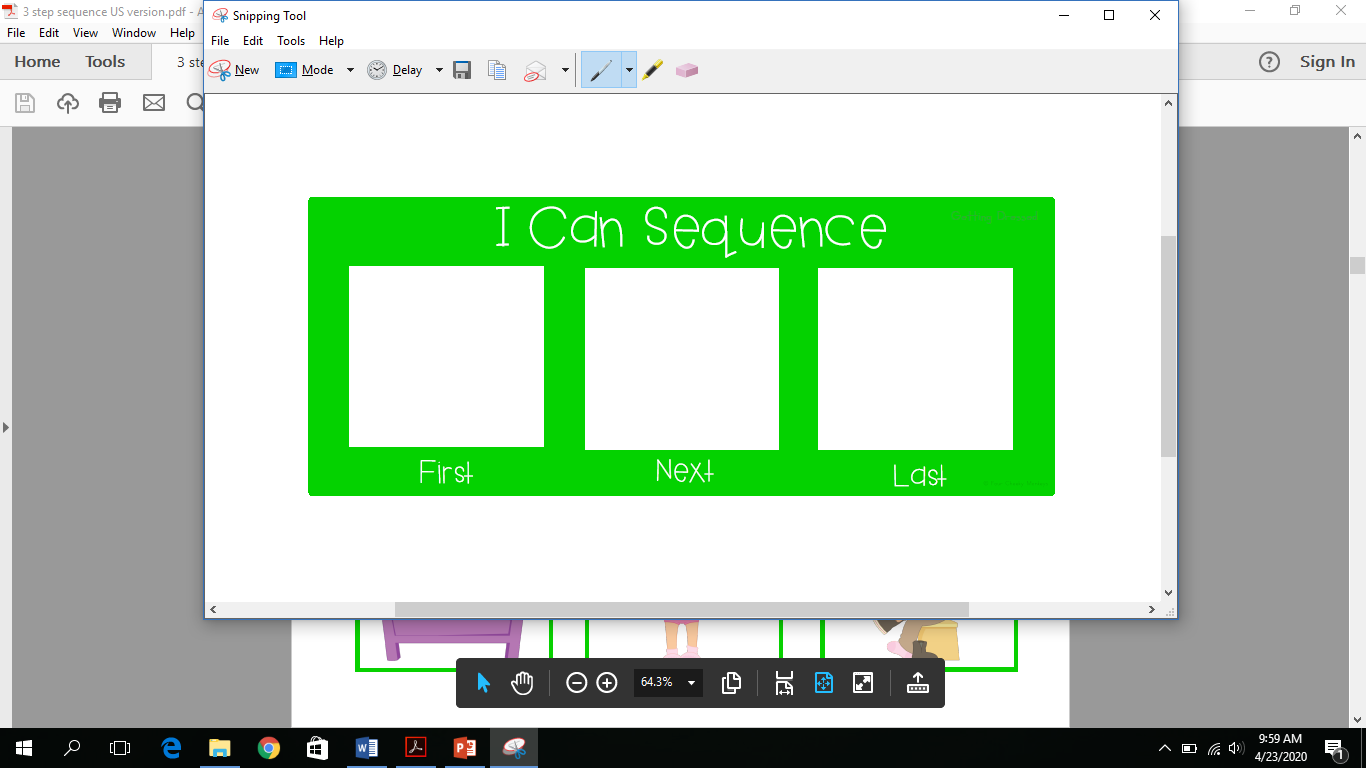 STEP 6: After this new window pops up, you can copy and paste the picture into your new blank document in Powerpoint. To cut and paste, right click and select “Copy”, to paste right click and select “Paste”. You can also select “Ctrl + C” for copy and “Ctrl + V” for paste. The Control (Ctrl) button is located on the bottom left portion of your keyboard. 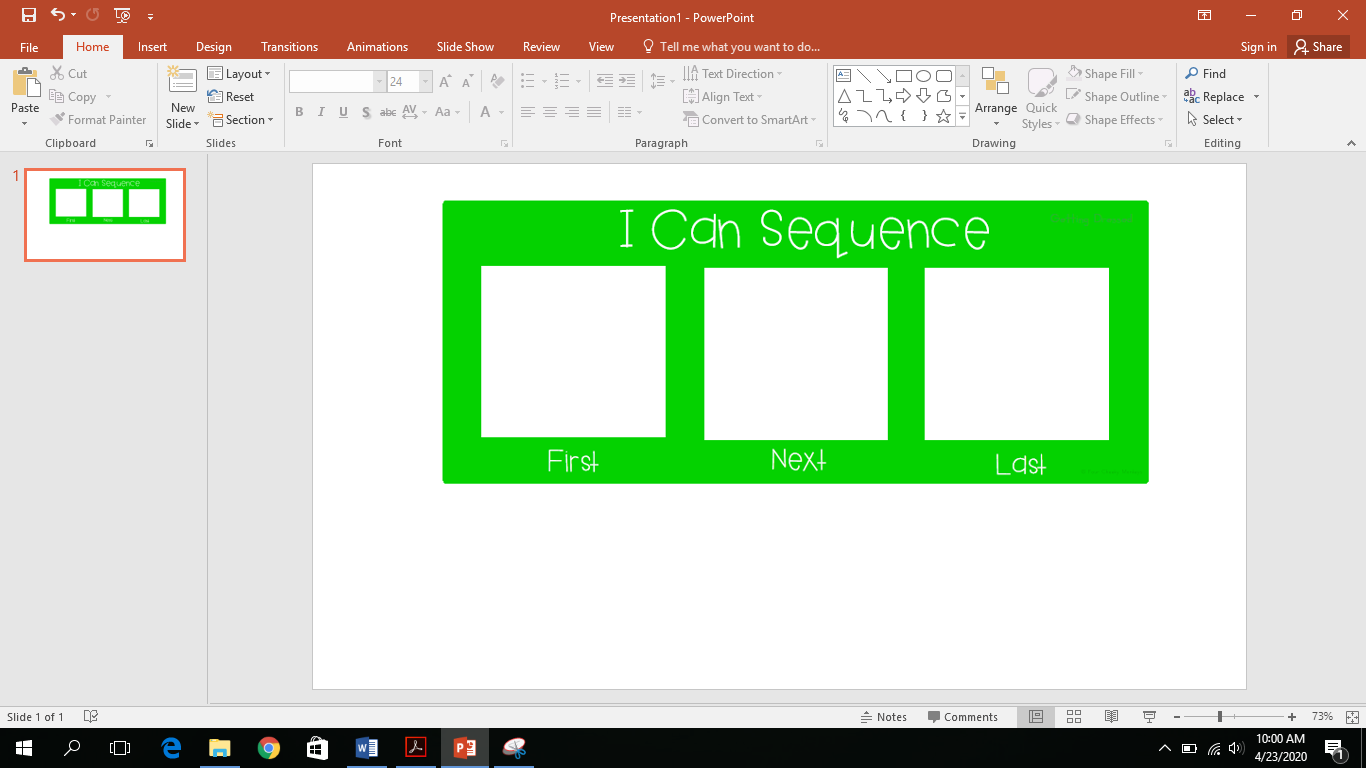 STEP 7: Go back and repeat Step number 4, 5 and 6 for any other areas of the PDF document that you wish to snip. I continued to snip the three sequencing pictures. 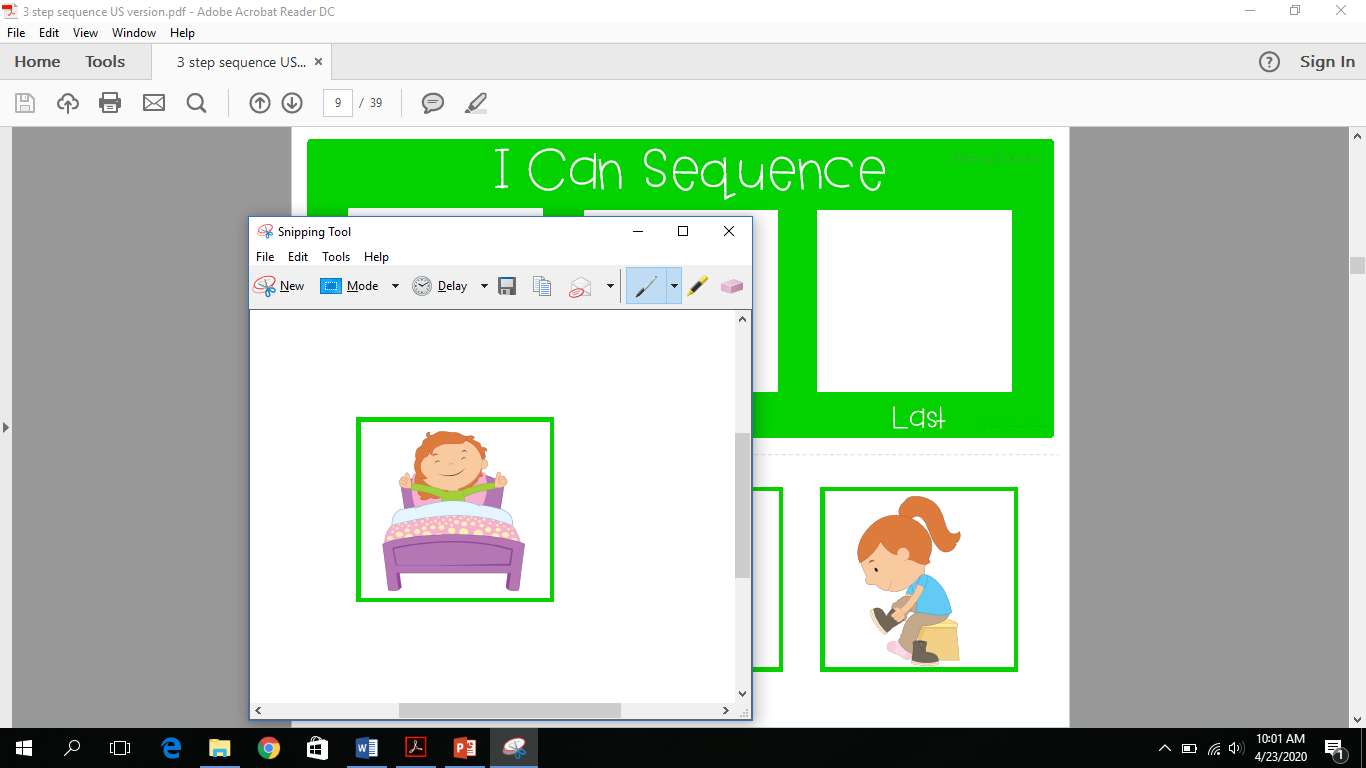 STEP 8: Once you have pasted all of the pictures into Powerpoint, it is now interactive and each piece can be moved around and manipulated. 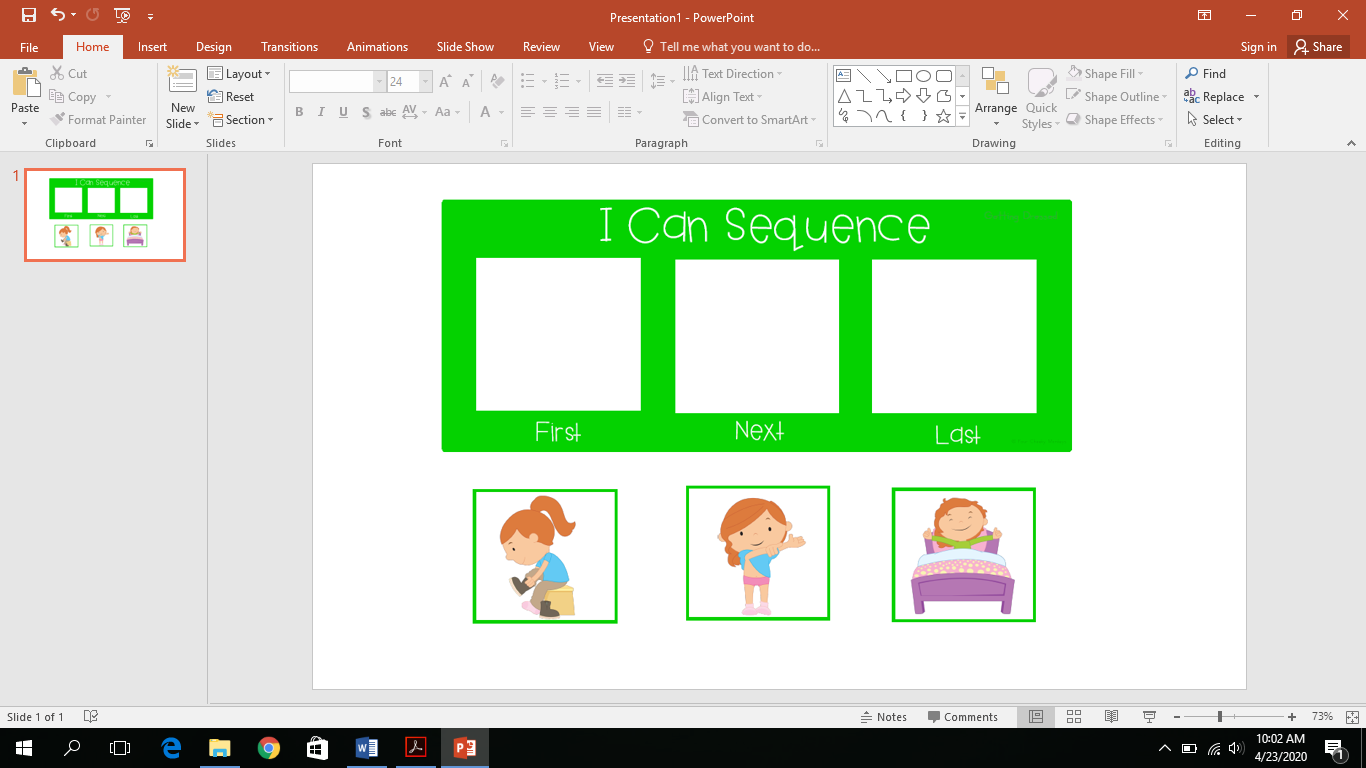 STEP 9: During a teletherapy session, you can now share your screen and have the student tell you which picture goes first, next and last while you move the pictures or if you can give the student mouse control they can put the pictures in the correct order themselves. 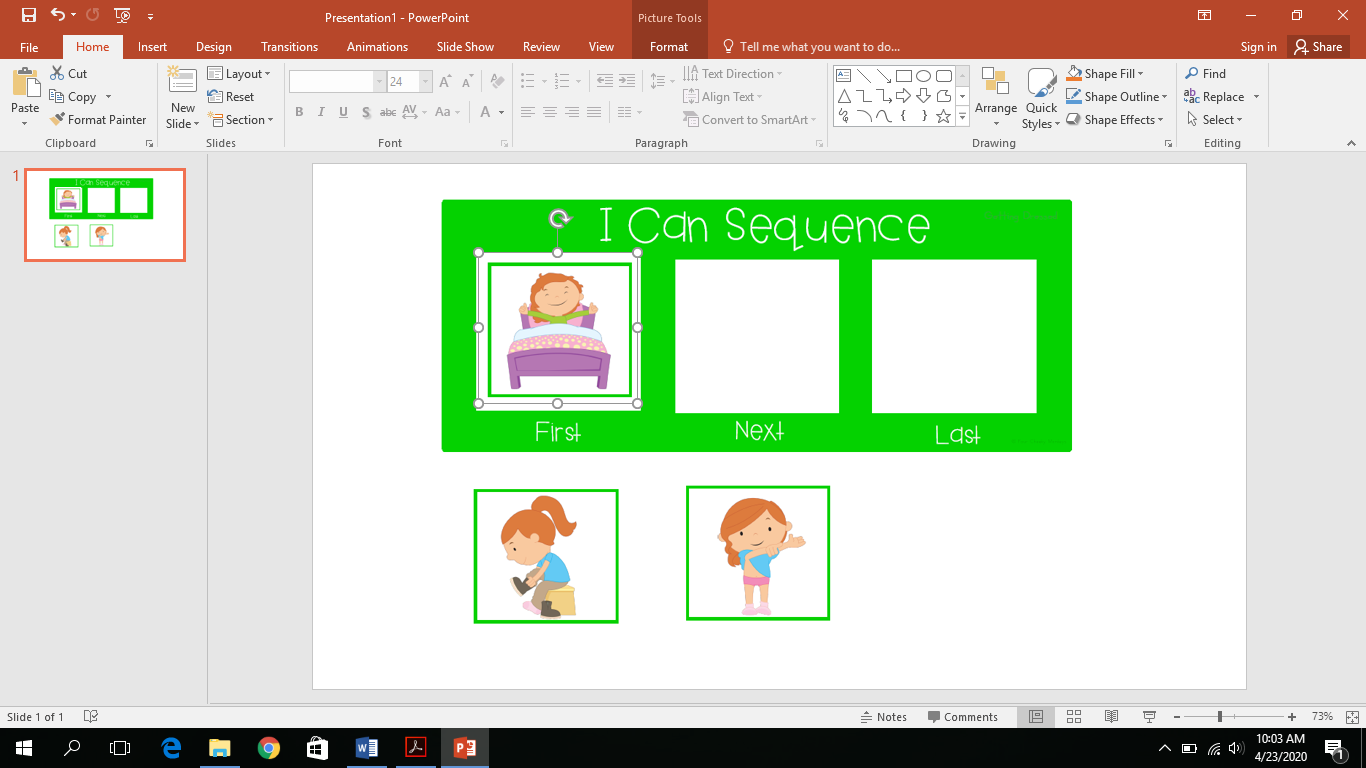 STEP 10: You can continue these steps and create an entire interactive document and then save it to your computer to easily open up during teletherapy sessions. 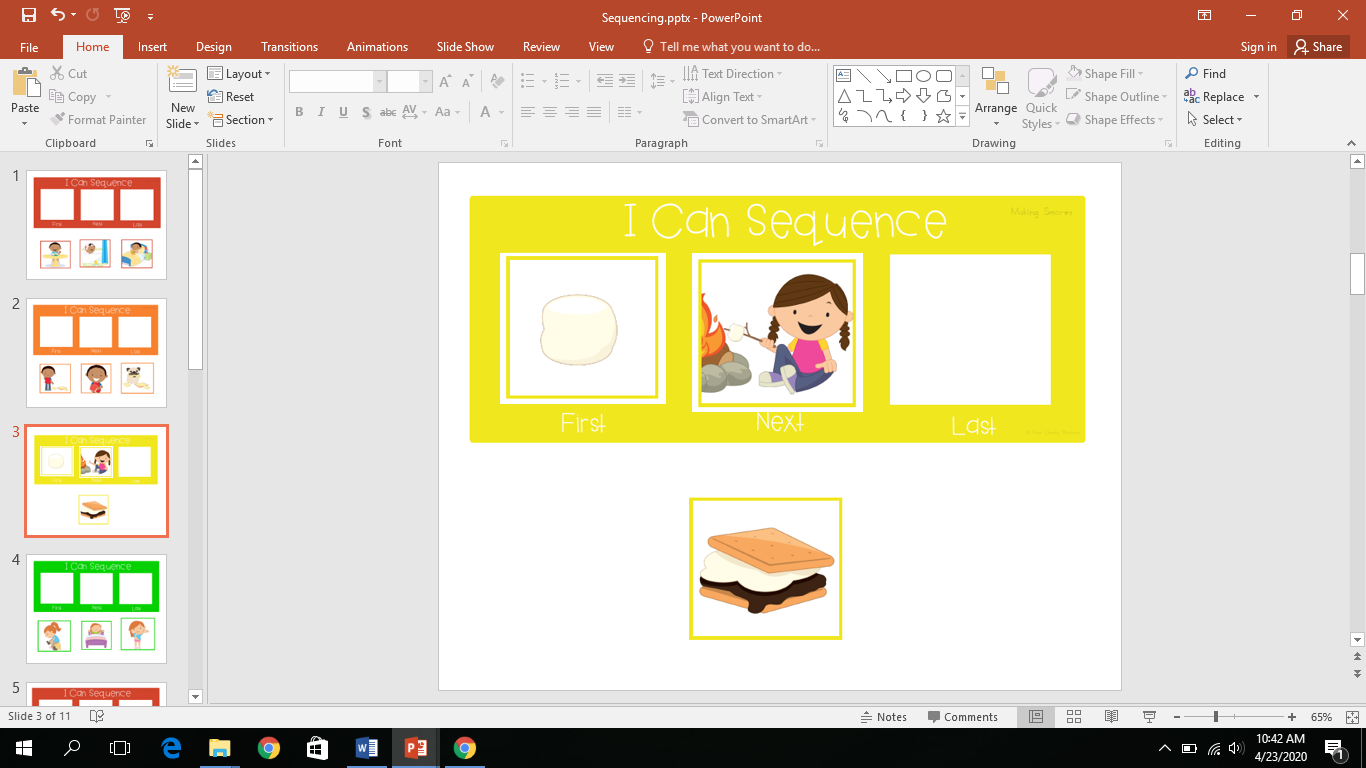 Determine your business structure. Research different business structures and speak to an accountant in your area. Business structures include a Sole Proprietorship, LLC, Corporation (C-Corp, S-Corp) and Partnerships. It is important to also be aware of your state rules and see what will work for you. For example a sole proprietorship costs less money, but comes at an expense of more liability. Ultimately, I went with a Sole Proprietorship because in the state of California they do not allow a single member LLC. If I could have, I would have went with an LLC since it is a flexible business structure and separates business and personal liabilities.
Determine your private practice model. Your choice for a business structure may also depend on your private practice model - are you only going to be seeing patients in their home? Are you going to open up a clinic and have an office-based practice? How big do you anticipate the clinic being? Is this going to be part or full time job? I chose to do in-home therapy since real estate is so expensive here in CA and I didn’t want to jump right into that. I initially wanted to see children in my own home, however after checking with local Zoning Laws, I found out my city doesn't allow that. So check Zoning Laws as well! Get Professional Liability Insurance if you don’t already have it. Popular companies for SLPs to use are: https://www.hpso.com/ and https://www.proliability.com/ Insurance or Cash Only? I chose to be a private pay only practice. Since this was a part-time job for me, I did not feel the need to contract with insurance companies (become an in-network provider) in order to obtain clients. This decision will also depend on projected scope of business and what disorders you intend to treat, experience (are you an expert in a particular area that families will seek out? Is your area of expertise typically reimbursed by health plans?), the affluence of your community, and the state of economy. If you decide to go with a cash only practice, you can provide families with documentation of your services to submit to their insurance companies. Make sure they sign a form indicating that they understand they are responsible for the payment even if they are not reimbursed by their health plan. I always require payment on the day of service or I have client's pay in advance for the month. Families can check with their insurance companies before beginning therapy services to see if their insurance company will reimburse for out-of-network benefits. If you choose to become an in-network provider with insurance companies, know that it takes a considerable length of time. The process of applying can take months. Submitting claims, determining eligibility, collecting co-payments and tracking payments also takes up a lot of time. For reimbursement purposes, you need to get an NPI number (National Provider Number) and this will identify you as a provider on claims you submit to insurance. For tax purposes, you may also need to obtain Tax ID number (EIN - Employer Identification Number) to receive payment from insurance companies to your business. (Even though I do not contract with insurance companies, I got an EIN number and file my taxes under that instead of using my Social Security number). Writing a Business Plan. If you are seeking a bank loan to start up your business, you will need to write a business plan. Consult with an attorney and accountant to set up your business and write your plan. Helpful websites include: https://www.sba.gov/ and https://www.score.org/ Determine a name for your practice. You can just use your own name if you choose to be a sole proprietor or decide on a company name as well that is different. I chose Gate to Communicate Speech Therapy as my business name and in order to do that I needed to get a business license with my city (~$130) and had to file a DBA (doing business as) with my county (~$35). It's important to research whether the name is already being used by others. If it is being used by others, you may have a difficult time getting the domain name that you want for your website and may confuse people. Ideally, choose a name that is not in use. You may also want to consult with an attorney to ensure whether your state has regulations regarding your name choice and if it needs to be approved. You can also ask about trademarking your logo or name. Remember your vision of your practice. If you open your practice as "Jane Doe, Speech Therapy Services" and then in a few years when the business is growing, you want to add employees you may need/want to rename your business and that can be difficult. You can check this website to see if a domain name is taken: https://www.name.com/domain/search Creating a website. Your next step is to look into creating a website for your business. In this day and age, most people find companies with a quick internet search, so a website is important. You have options of using SquareSpace, Weebly, Wix, Wordpress, GoDaddy etc. I chose Weebly and found it very easy, great customer service and price was good. Also make sure you get on Google My Business, so you pop up when customers search your area for speech therapists. Get a business email. You can get a HIPAA compliant email by signing a BAA through G Suite and this will give you a more professional looking email @yourdomainname such as [email protected]. I also have seen practices who use a typical email at gmail.com as well. If you are not transmitting personal health information or client information, this may be okay. You can also look into: Hushmail, and ProtonMail. Get a business phone number. You can use your personal phone number or get a different business phone number. I set up a free google voice number with an area code of where my business is. I did this because my regular phone number is where is grew up in NY and wanted the area code to be in the area I am currently servicing. You can also look into: Spruce Health, Grasshopper, Sideline and Line2. Get a business bank account. Make sure your business income is separate from any other income or money in your bank. I did not specifically set up a "business bank account", I just changed my second savings account that I already had open to be named "business" and this is where I transfer all business income. Paper documentation or EMR Software? What are you going to do about documentation? If you decide on paper reports, SOAP notes, invoices, etc then get a locking file cabinet and place it in a locking room in your household for HIPAA compliance. If you are looking into EMR softwares for paperwork, scheduling, billing, etc. Look into different choices: Simple Practice, WebPT, Office Ally, TreatWrite, Fusion Web Clinic, TheraNest, ClinicSource, Raintree, Practice Fusion, My Client Plus, Practice Perfect. I do not have an specific recommendations as I do not use an EMR system. Create your forms: Client intake forms, case history/developmental history, informed consent/authorization to treat, email/text agreement, payment policy, cancellation policy, video release, release of information, How did you hear about us, HIPAA forms, SOAP note document, Superbill etc. Attached is ASHA's example of a Superbill for SLPs: https://www.asha.org/Practice/reimbursement/coding/Superbill-Templates-for-Audiologists-and-Speech-Language-Pathologists/ Set your hourly rate: For your payment policy, you will need to list your hourly rate. You can look to see what other therapists in your area charge and see what the typical price range is. Just avoid discussing rates with other providers as it can be construed as price fixing. This will also vary based on expertise and experience. Decide on payment method: Will you accept cash and check only or do you want to accept credit cards? For the first two years, I only accepted cash and check. I now use IvyPay for credit cards since parents definitely prefer to have their card charged then to have cash on hand or writing a check each session. You can also look into Square, PayPal Business, Zelle, Wave App, Quickbooks, Authorize.net, Freshbooks, Go Card Connect are a few others that I have heard of, but do not use. Determine your niche. I believe it's best to focus on a specific area in our field or population and market yourself that way. Ages, population, disorders, etc. (e.g. children, preschool age, fluency disorders). Have a goal of becoming the go-to person in your area for that disorder. Creating business cards/logo. I had cards made on Vistaprint and had my friend create my logo. For business cards check out: Vistaprint, Moo, Zazzle, Staples, Canva or Makr and for Logos check out: Fiverr, Instalogo, Canva, Vistaprint, Etsy, 99 designs. Buy assessments. After you determine your population, age range and disorders that you will be working with invest a few assessments. Look into Q global for online assessments. Also be sure to look into free assessments such as the Communication Matrix. Fax options: If you are in need of a way to fax items check out: sFax, Filesanywhere, Faxage, Ring Central Fax, Nextiva Fax, eFax, SRFax, Genius Fax and Smart Fax Side note: If you are a sole proprietor, you may want to get a P.O Box with a real address for your business so on your paperwork you can put that address instead of your home address. With getting an NPI, EIN number, and listing on all different websites your address begins to be plastered all over the internet and it's difficult to get rid of. Marketing:
Hope that was helpful to get you started! The Principles of Motor Learning are a set of processes that facilitate the acquisition and retention of motor skills.
Motor Performance - The ability to perform a motor task. How the movement is performed during training, within a structured session. (Temporary change during the speech session). Motor Learning - Retention and generalization (transfer) of skills learned including how the movement is performed at another time or in another setting outside of speech therapy. The process of the learner acquiring a skill and making a movement automatic. Precursors to motor learning in young children:
Conditions of Practice Target Choices/Target Complexity (Type, length, phonetic complexity)
Practice Amount: Small vs Large Refers to the amount of time spent practicing movements
*Maximum response trials - Attempt 50-200 trials depending on the severity of the disorder. *Larger number of trials leads to greater retention and generalization (Edeal & Gildersleeve-Neumann, 2011). Practice Distribution: Mass vs Distributed practice
*Distributed practice leads to better retention and generalization of a skill (Bahrick & Hall, 2005). *Typically in children with CAS, distributed practice over time (4 sessions a week for 20 minutes) appears to be more beneficial than massed practice (1x a week for an hour). *Massed practice may look like working on 3 targets for 4 weeks, and then 3 novel targets for 4 weeks, rather than 6 targets for 8 weeks straight. Practice Schedule: Blocked vs Random practice
*Evidence shows random practice leads to better motor learning and generalization (Shea et al., 1990), but for more severe cases, blocked practice may be necessary at first to optimize learning. *If you start with random practice then it will take the child longer time to acquire the accurate movement gesture for that target. *One study in CAS treatment (~2.5hr tx/week, 2-4 week phases): 2 children showed greater retention with blocked, 1 child showed greater retention with random and 1 child showed no clear improvements with either condition (Maas & Farinella, 2012) . Practice Variability: Constant vs Variable practice
*Constant practice is better for acquisition of a skill and may be better for learning the underlying timing pattern of a motor program (Lai et al., 2000). *Variability can also include working on prosody to practice more flexibility in motor planning and programming as well changing stimuli (orthographic vs picture), changing carrier phrases or even changing the setting. Conditions of Feedback (Type: Knowledge of Results/Knowledge of Performance, Frequency: High/Low, Timing: Immediate/Delayed) Feedback Type: Knowledge of Results vs Performance
*To promote generalization and retention of a motor skill, move to knowledge of results feedback. Feedback Frequency: High vs Low
*More frequent feedback might be required initially for learning of complex skills. Begin with more feedback and gradually fade to less, so a child does not rely on this. *Children may benefit more from more high frequency feedback overall (Sullivan et al., 2008). *Few studies have examined feedback frequency in speech motor learning. *One study with children with CAS (Maas, Butalla & Farinella, 2012) showed 2 children with greater retention with low frequency feedback, 1 child with greater retention with high frequency feedback and 1 child with no improvement in either condition. (High frequency feedback meaning feedback given on 100% of trials, low frequency feedback meaning feedback given on 60% of trials). Feedback Timing: Immediate vs Delayed
References: Maas. et al. (2008). Principles of Motor Learning in Treatment of Motor Speech Disorders. American Journal of Speech-Language Pathology, 17, 277-298. 1.) How many SLPs are in the district? Are most SLPs district employees or contractors?
2.) Do I need a teaching credential or any other credential? 3.) Is there a budget for materials or are there materials provided at each school? CEUs/Conferences reimbursement? 3.) Will I have my own classroom/room/space or sharing a space? 4.) Are supplies available at school such as paper, markers, sticky notes, etc? Printer? Color copying? Laminating? 5.) Do I get a computer to use or have to use my own? 6.) What are typical caseload numbers? Average at each school? 7.) Will I be the only SLP at the school or will there be others? 8.) What assessments are available to us? What assessments will be available at my school? 9.) Will I be servicing General Education students only? Special Day Class students? What Special Day Classes are in the district? (Mild-moderate, moderate-severe, Autism, Emotional Disability, Behavioral, Medically Fragile? etc.) 10.) What ages will I be working with? Will I be working with preschool as well? 11.) Is there a preschool assessment center or will I be conducting preschool assessments? 12.) What IEP system does the district use? Will training be provided? 13.) Am I paid on a "therapist" salary or a "teacher" salary? 14.) Do previous years at another district count? What salary step would I go in at? 15.) Socioeconomic status of the students/families i'll be working with? 16.) In what instances do I have to "make up" sessions? 17.) Will I have SLPA support at my school? 18.) Benefits? 401k, 403b available? If I work part-time, can I still receive benefits? 19.) How many days off will I get per school year? Sick days versus PTO? Summers off or year round school? 20.) Does the district use Response to Intervention? Who can be put on RTI? (e.g. students working on articulation only or language as well?) 21.) What program is used for billing? Do we use paper or electronic billing? 22.) Who is responsible for documentation and billing? Is it the SLP or is someone else brought in to complete this part? 23.) How many high profile IEPs at my assigned school? Are there any litigation cases with any students on my caseload? 24.) Will I be at one school or more than one? 25.) Will I have to change schools mid year or stay at 1 school full time for the whole year? 26.) Do you try to keep SLPs at the same school year after year or will I be moved around? 27.) What other responsibilities will I have at my assigned school? (e.g. bus duty, recess duty, joining a committee) 28.) Will I be evaluated? How often? 29.) Will I have to see students outside of school or evaluate private school students off campus? 30.) Am I paid overtime? 31.) School hours? What are my duty hours? 32.) Will my be license be revoked if I break my contract early? How long is my contract for? 32.) Who will I be the case carrier for? Speech only students or other students as well? 34.) The caseload limits in this state are --, will this number be enforced? Will extra support be provided when that number is reached? 35.) Are IEP meetings before/after school hours or during the day? While speaking to several parents over the years, I have realized that early on in the evaluation process, the majority of parents do not understand that there is a difference between "speech" and "language". "Speech" is an omnipresent term that is used to describe therapy services. Most people refer to services as "speech therapy" "speech services" or seeing a "speech therapist", however our technical term in the United States is a Speech-Language Pathologist due to the fact that speech and language are two distinct areas. At times, a child may need to work on both speech and language, however a lot of the time it's one or the other that is being targeted.
What is Speech? Speech refers to a neuromuscular process by which we turn language into a sound signal that is transmitted through air. It is the physical aspect of talking and how we say sounds and words. It incorporates using muscles including the tongue, lips, cheeks, jaw and vocal tract to produce intelligible words. What is Language? Language refers to a system of conventional spoken or written symbols (including written, spoken or expressed through gestures and body language) used by people in a shared culture to communicate with one another. It is the words we use and how we use them to share ideas and get what we want. Language consists of:
What is Communication? Communication is the process of conveying a message and sharing information among two or more people. It must have a sender and a receiver as well as involve formulation, transmission, reception and comprehension of a message. Which disorders fall under the category of "speech"? Articulation Disorder – This is a label given to children who demonstrate sound production errors that do not affect meaning. These speech sound errors may consist of omissions, substitutions, distortions or additions. (e.g. children who say "wion" for "lion" or children who have a lisp). At a young age, it is common for children to have difficulty producing various speech sounds. There are several charts online to look at to see which errors are age appropriate. Phonological Disorder – This is a language based disorder that presents itself in the area of speech. If a child is diagnosed as having a phonological disorder, it means the child is having difficulty understanding the sound system and using speech sound patterns correctly in a language. They often do not use some or all of the speech sounds to form words as expected for a child their age. It is a speech simplification process that results in a collapse of phonemic contrasts which affect meaning. (e.g. a child is consistently dropping the "s" in s blend words (pin for spin OR nap for snap), yet they can correctly produce the "s" sound in other contexts such as "sock"). Stuttering- Fluency is the overall rate of speech. Stuttering is classified as an abnormally high frequency and/or duration of stoppages in the forward flow of speech. Childhood Apraxia of Speech (CAS) – This label is given to children who have the inability to plan and execute volitional motor movements in spite of intact muscle strength and coordination. With CAS, the brain has difficulty with developing the motor plan for speech movements as well as a disconnect when sending the message from the brain to the muscles of the mouth. This may impact speech production and prosody. Dysarthria - Dysarthria is characterized by impaired muscular control over the speech mechanism. With Dysarthria, the motor plan for speech correctly gets sent to the mouth, however an individual has difficulty executing the speech movements due to muscle weakness. Voice Disorder - This refers to the overall quality of one’s speech. A voice disorder includes abnormalities in the production of sound by the larynx involving pitch (high/low), volume (loudness/softness) and other qualities of your voice. Examples of various vocal qualities include: strain/strangle, breathy, hoarseness, harsh, nasal, gurgly and tremor. Orofacial Myofunctional Disorder - The Oral Peripheral Mechanism (OPM) refers to the oral structures including lips, teeth, tongue, jaw and palates involved in verbal production. Orofacial Myofunctional Disorders refer to disorders of the muscles and functions of the face and mouth. It involves abnormal movement patterns of the lips, jaw or tongue during rest, swallowing or speech. Which disorders fall under the category of "language"? Expressive Language Disorder - Expressive language is the output of language consisting of speaking and writing. These skills are a child's ability to organize and use spoken language to express their wants, needs, thoughts and feelings. It also includes their ability to use age appropriate vocabulary and follow the rules of grammar, which dictate how words are combined into phrases and sentences. If a child is struggling in this area, it is referred to as an Expressive Language Disorder. Common issues being: a child is not using words to communicate, not combining words into phrase/sentences, not using beginning/endings of words, not using appropriate sentence structure. Receptive Language Disorder - Receptive language refers to the understanding of language or the input of information consisting of listening and reading. These skills include a child's ability to understand spoken language by processing sounds, words and sentences, retrieving words and information, and understanding vocabulary, grammar and sentence structure. If a child is struggling in this area, it is referred to as a Receptive Language Disorder. Common issues being: not following directions, not answering questions when asked, appearing confused when told something. Social (Pragmatic) Communication Disorder - Pragmatics refers to the rules that govern and describe the use of language in communicative interactions, including the social aspects of language. These includes social skills, such as, when it is an appropriate time to say something, what words to use, or how to say something in a given context. Pragmatics also incorporates using appropriate body language and non-verbal communication as well as interpreting other's body language and responding to social cues. You can have speech without language - Think about a toddler using jargon. The toddler is physically speaking, however we do not understand what they are saying. You can have language without speech - Think about American Sign Language (ASL). ASL is a true language shared by a certain culture that is governed by particular rules, however involves no speaking. You can communicate without speech or a shared language - Think when you are in a foreign country and you do not speak the same language. You communicate through nonverbal communication such as pointing, body language, facial expressions, drawing pictures, etc. For more information, check out: https://www.asha.org/public/speech/disorders/ChildSandL/ https://www.asha.org/public/speech/development/speech-and-language/ Simple Social Interactions - You don't always need toys to interact and play with your child!4/1/2019  Lets admit it, toys are sometimes a hassle, you pay a lot of money for a toy and your child doesn't like it or they get bored after one time playing with it. We've all been there and it's frustrating! Well the good news is, you don't always need toys to interact and play with your little one! There are several toy free "games" that consist of two people interacting with each other that are just as fun and engaging. The social interaction games listed below are great for building speech, language and of course social skills! You can focus on making eye contact, joint attention, turn-taking, requesting, imitation of actions/nouns and much more! As a speech therapist, I work with many children who have a difficult time with social reciprocity and engagement. The child is often lacking those joint attention skills (looking at an object, then at the person, and back to the object) during interaction and play time. I have found that these toy free social interaction "games" work wonders and almost always get the child more engaged with me!
Some examples of social interaction games include:
Children are always craving movement and they are naturally drawn to variations in pitch, intonation, and loudness in our voices, so it is important to move around, be fun, act silly and incorporate sound effects during these games. This will facilitate the interaction between the two of you! Enjoy! What is Childhood Apraxia of Speech?
"CAS is a neurological childhood speech sound disorder in which the precision and consistency of movements underlying speech are impaired in the absence of neuromuscular deficits (e.g., abnormal reflexes, abnormal tone)..." (ASHA, 2007a, Definitions of CAS section, para. 1) What to look for… 10 Core Characteristics of CAS: 1.) Inconsistent errors on consonants and vowels in repeated productions of syllables or words 2.) Lengthened and disrupted co-articulatory transitions between sounds and syllables and difficulty with initial artic configurations 3.) Inappropriate prosody, especially in the realization of lexical and phrasal stress (robotic sounding, difficulty with intonation, rhythm, lack of variation in pitch or ability to control or decipher loudness) 4.) Consonant distortions 5.) Vowel errors – substitutions and distortions 5.) Groping 7.) Intrusive Schwa 8.) Brief or inappropriate pauses 9.) Slow rate of speech and increased difficulty with multi-syllable words 10.) Voicing errors (ASHA; 2007; Davis, Jacks & Marquardt, 2005; Iuzzuni-Siegel et al, 2015; Shriberg and Strand, 2014) A dynamic assessment is essential for a differential diagnosis of CAS! Where to begin... Assessment
Motor Speech Evaluation Determines motor planning ability for speech
Continuation of Assessment
For a more thorough assessment checklist, checkout my Teachers Pay Teachers store at www.teacherspayteachers.com/Product/Dynamic-Assessment-for-Childhood-Apraxia-of-Speech-Checklist-4438888 I find that my student's tend to engage a lot more if we are doing something in therapy that can exert their energy along with practicing their speech and language goals. It makes it more fun for them and can lead to better generalization of a skill if the student can practice that particular skill in context. Such as, if practicing the CVC word hop, have your child hop while practicing the word instead of just sitting at a table saying the word over and over again. Below are three other ways to make speech therapy sessions up and about: 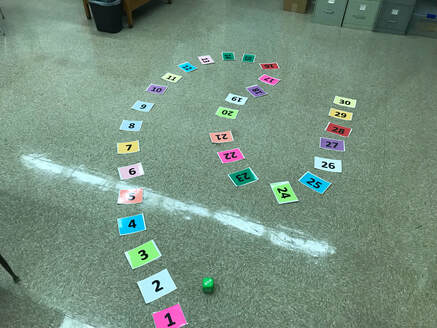 Human Game Board Just like how you would play a board game at the table, print off number cards and do a human game board instead! The kids will enjoy it way more. After each turn, have them practice their particular speech or language skill that you are working on. Often I will put a small prize at the end and when they finsih the game board they can choose one (a sticker, pencil, eraser etc.) 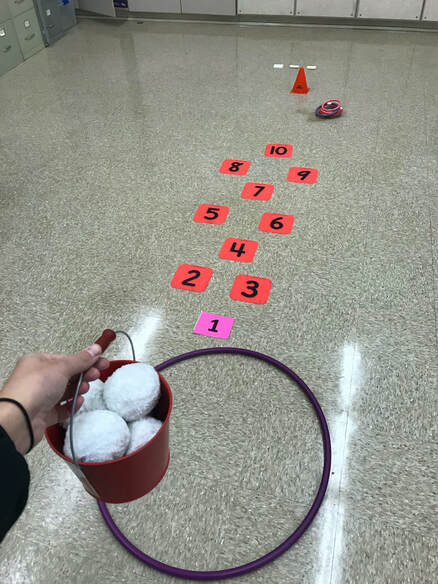 Obstacle Course Here I've made a small obstacle course the children have to get through which includes throwing a snowball into the hula hoop, doing hopscotch and then getting a ring on the ring toss. Once they go through the obstacles, they pick up a sticky note which contains their targeted word, or what they are working on in speech. You can easily vary this and adapt it in any way needed.
Do a scavenger hunt! It can be inside or outside depending on accessibility at your facility/school. Above are two free scavenger hunt lists on www.teacherspayteachers.com - links below. You can make your own scavenger hunt in anyway - such as find 5 objects in the room that start with the letter "s" and then practice those words. If working on categories, hide items around the room and ask the students to find 3 animals, 3 vehicles, 3 toys etc. Hope this blog post sparks some ideas in your head on ways to make your therapy sessions more fun for your students, yet just as engaging!
https://www.teacherspayteachers.com/Product/Speech-and-Language-Nature-Scavenger-Hunt-FREEBIE-2515588 https://www.teacherspayteachers.com/Product/Scavenger-Hunt-Targeting-Basic-Concepts-3961151  "Before words and sentences emerge, a child needs to possess the ability to imitate. A child needs to react to events going on in their environment and be able to imitate those various actions/gestures and sounds that he/she sees through out their day. Other important pre-linguistic skills include joint attention, eye contact and attention. Exclamatory words quickly draw attention and engage little ones. They can easily be used during play time and in every day routines for a fun and functional way to build and expand your child's language skills as well as develop a larger repertoire of speech sounds. Below is a list of various exclamatory words that can be paired with different objects, which can easily be incorporated into play time with a child. "mmmm" "yummm" "ick" "ew" "blah"- These can be used when feeding stuffed animals or a baby doll. Another great activity is using velcro fruit & vegetables and then pretending to eat them. Pretend the foods are good and say "mmm" also pretend they are yucky, spit it out and say "blah!" - kids love this one! "vrooom" "errrr (screaching)" "boom!" "beeep" "crashing noise" "whoa" "choo choo"- Vehicle noises "weeee" "uhh ohh" "ouchie" "ow" "woohoo" "yippee" "oopsie" "lalala/singing sound" "mwah/kissing sound" "hmm/thinking sound" "ughh/mad sound" "wow" "nigh-nigh" "yay" "gulp /drinking noise", "shhh" "wahhh/baby crying" "aww" "eek!/scary sound" "aahhh/scary sound" "boo" "tah-dah" "pee-u"- These can be used when playing with toy people and using accompanying items. Such as saying 'weee' down the slide, 'uhh ohh" when someone falls down and "eek! when making a scared face!" "ahhh choo" - Kids love fake sneezing! Place toys on top of your head and pretend to sneeze and I'm sure your little one will get a kick out of it. "popping sound with lips" - Use this with bubbles. "whoosh" "boing" - Playing with a toy ball. Animal sounds: "oooh oohh ah ah for monkey" "buzzzz for bee" "moo" "neigh" "oink" "baaa" "ruff ruff" "h-h-h- as panting dog" "meow" "heee/ hissing cat sound" "quack" "cockadoodledooo" "roar" The book Moo Baa Lalala By Sandra Boynton is a boarded sturdy book that comes in a small size or lap size that is great to use with toddlers to work on animal sounds. Using all these exclamations with different objects can be used to establish joint attention with your child (shifting the child's focus from you to the toy and back to you) as well as establish eye contact and attention. It can also be great to build functional play skills and using toys appropriately and facilitate reciprocal play. When using these exclamation words use a slower rate of speech and vary your pitch and intonation. Overemphasize vowel sounds and syllables. Children are naturally drawn to our voices and are more likely to attend to varying intonation with excitement. Make sure you are really engaging with your child and looking them in the eye. Always accompany gestures as well with the sounds to facilitate imitation of these actions. For children with delayed language and late talkers, use toys that are your child's favorites. Follow your child's lead with which toys they choose and what they want to do with those toys. From here, pause and wait. Repeat the exclamation several times for more exposure to the word to facilitate verbal imitation. Try to avoid telling your child to "say weee!" etc. Praise any attempts including gestures. For children with Childhood Apraxia of Speech, hold the objects right next to your mouth when saying the sounds. These individuals often have difficulty with coarticulatory transitions, so placing the object at your mouth will focus their attention there. This way they can watch your mouth as you make the noises. Make sure to keep the sounds together and stretch the word out, do not separate them. With CAS, the focus is on movement. (e.g. cow says "mmmmoooo" - not mmm...oooo. Also vary prosody - say sounds in a "mommy /daddy/baby voice" "high like a mouse/deep like a lion voice", or excited/sad/mad voice. For children with severe speech sound disorders and articulation errors, make sure to extend the vowel sounds when using these exclamations. Vowels sounds contribute more to intelligibility than consonant sounds do. Prolonging the vowel sounds gives more time for your child to think about the consonant sounds that follow as well. Children learn through play! Remember, they don't like to listen to us, they like to imitate us!  |

|
Photo from Carla216
